Kim M, et al. | Int J Radiat Oncol Biol Phys. 2025 13
A prospective study evaluating TTMV-HPV DNA kinetics during chemoradiotherapy. Week-4 TTMV decline correlated significantly with primary tumor volume reduction and nodal response on mid-treatment MRI/PET imaging, providing quantifiable, real-time evidence that TTMV clearance mirrors early tumor response while treatment is still ongoing and potentially modifiable. This study supports the clinical rationale for serial TTMV testing at the mid-treatment timepoint.
Huttinger L, et al. | Oral Oncology. 2025 | N=17 50
Evaluated TTMV-HPV DNA as a predictive biomarker during induction chemotherapy (IC) for HPV+ OPSCC. TTMV clearance after the first IC cycle predicted final disease control with 61.5% accuracy vs. only 7.7% for PET-CT (p=0.01), a striking demonstration that molecular response outperforms imaging at this early timepoint. Critically, all patients with elevated TTMV after completion of CRT had persistent disease: 100% concordance, establishing residual TTMV as a near-definitive marker of treatment failure in this setting.
Routman DM, Kumar S, et al. | Int J Radiat Oncol Biol Phys. 2022 | N=105 49
In 105 HPV+ OPSCC patients treated with CRT, persistent or rising TTMV-HPV DNA at the end of treatment strongly predicted locoregional recurrence and worse overall survival. Patients who achieved TTMV clearance by end of CRT demonstrated excellent disease-free survival — establishing end-of-CRT TTMV status as a clinically meaningful indicator of treatment success and a signal for heightened post-treatment surveillance in those who do not clear.
Chera BS, et al. | Clin Cancer Res. 2019 | 3-year longitudinal 7
A 3-year longitudinal study demonstrating that rapid TTMV-HPV DNA clearance kinetics, defined as >95% decline by week 4 of CRT, were associated with improved long-term disease control. This foundational study established the mechanistic framework for TTMV clearance as a treatment response biomarker during CRT and provided the evidence base for subsequent prospective work on clearance-guided risk stratification.
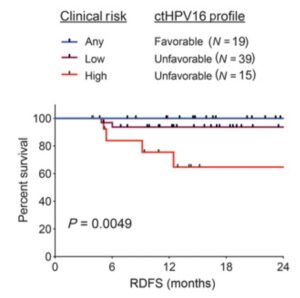
A favorable circulating TTMV-HPV DNA clearance profile correlates with disease control in OPSCC patients treated with CRT. Kaplan–Meier analysis of RDFS stratified by clinical risk and ctHPV16DNA profile. P value calculated using a two-tailed log-rank test for trend.
Chung CH, et al. | Clin Cancer Res. 2022 52
A phase 1/2 prospective trial evaluating cetuximab + nivolumab in recurrent/metastatic (R/M) HPV+ HNSCC. Serial ctHPVDNA measurements preceded imaging confirmation of both response and progression — rising ctHPVDNA indicated disease progression and declining ctHPVDNA indicated treatment response, both before CT or PET/CT confirmed the change. This is the first prospective pharmacodynamic biomarker evidence supporting ctHPVDNA monitoring during systemic therapy in R/M disease and was cited by the CHNC as the basis for their M1-setting consensus statement.






