



HPV+ Oropharyngeal Cancer
NavDx® Testing in Surveillance.
Performance at a Glance.

Standard OPSCC Surveillance Has Limitations.
Physical exams, nasopharyngeal endoscopy, and imaging have long been the standard of care for post-treatment OPSCC surveillance, but their ability to detect recurrence early is limited by several factors:
-
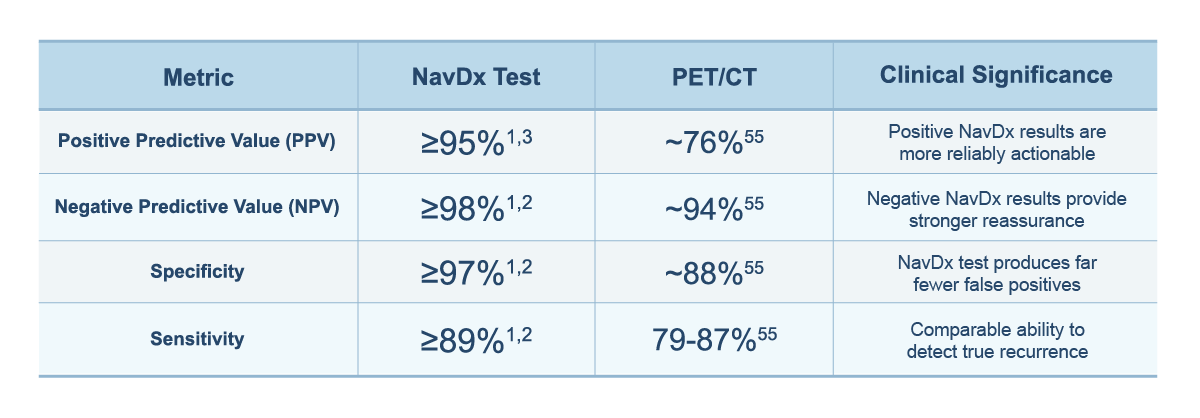
- With a PPV of ~76%55 and specificity of ~88%55, PET/CT positive imaging findings may not represent true recurrence. This could drive unnecessary biopsies, repeat imaging, and patient anxiety.
- Anatomical changes from surgery and chemoradiotherapy complicate the predictive value of physical exam, nasopharyngeal endoscopy, and imaging1
- Imaging can only detect locoregional tumors that have grown to a detectable size and may miss distant metastases outside the field of view42
- Nasopharyngeal endoscopy identifies recurrence in only 0.3–9% of surveillance visits11,56
The NavDx test operates at the molecular level and can detect TTMV-HPV DNA fragments in the bloodstream before tumors grow large enough for imaging or exams to find them, and without the false-positive burden that makes imaging findings difficult to act on.
Bringing Greater Precision
to HPV+ Cancer Surveillance.
The NavDx Test vs. Standard Surveillance.
Published data1,2,3,55 demonstrate that NavDx testing can substantially outperform PET/CT, particularly in positive predictive value.
Earlier Detection of Recurrence.
Published data demonstrate that NavDx testing can detect molecular evidence of recurrence a median of 4 months earlier than PET/CT or clinical exam.6,8 This lead-time advantage has direct clinical implications:
- 15–25% of HPV+ OPSCC patients experience locoregional or distant recurrence after treatment3
- In published research, 69% to 72% of recurrences were asymptomatic at first NavDx detection. Patients felt well and had no clinical findings; NavDx testing found disease before anything else did.2,3
- Experts have reached strong consensus that earlier identification of locoregional or distant recurrence may improve outcomes by expanding salvage therapy options, including surgical salvage.11
Resolving Clinically Indeterminate Findings in OPSCC.
Standard surveillance generates significant diagnostic uncertainty. Published research shows that across 543 patients at 8 U.S. institutions, 38.7% had at least one clinically indeterminate finding (CIF)—33% from exam, 67% from imaging, with 503 total indeterminate episodes. CIFs were most common in the first year post-treatment (2.1× higher odds in year 1, primarily at 3–6 months).39
- NavDx testing in the CIF setting demonstrated 97.5% overall resolution accuracy.39
- When NavDx testing was positive in a CIF context, 100% of cases were confirmed recurrences (19/19).39
- When negative, 96.7% were confirmed NED (60/62).39
- A positive NavDx result in the setting of an indeterminate clinical finding reduced median time to confirmed diagnosis from 97.5 days to 14 days.39
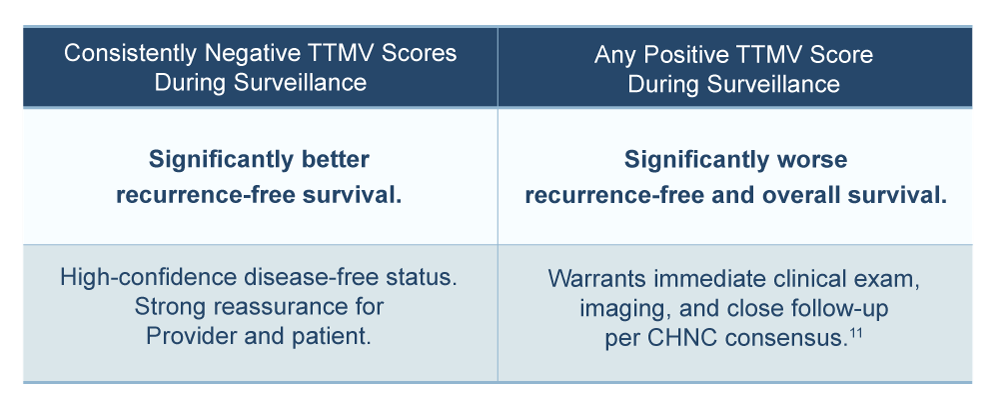
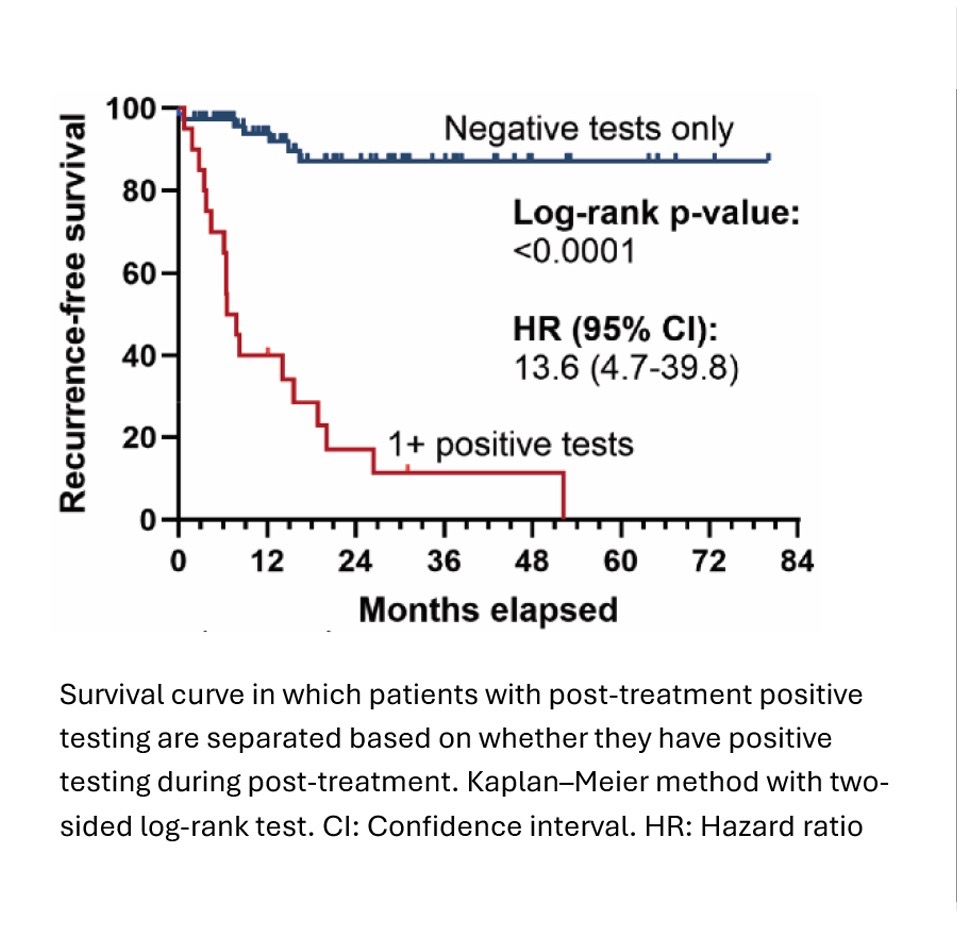
Survival Impact: What a Positive Result Means.
The survival data from Hanna/Roof 2023 provides important clinical context for interpreting a positive NavDx result during surveillance:
Lang Kuhs et al notes, “Survival after recurrence is significantly better for patients with a single focus of disease and those able to undergo surgical salvage treatment, suggesting that identifying recurrences early may prolong the disease-free interval, with potential for cure in a subset of cases.” 44
Berger BM, Hanna GJ, et al. | Clin Cancer Res. 2022 | N=1,0763
In this large multi-institutional retrospective study, 1,076 patients were tested during post-treatment surveillance. Of the 80 patients (7.4%) who had at least one positive TTMV Score:
- 59 patients (74%) had either indeterminate (IND) or no evidence of disease (NED) clinical disease status at the time of their positive test
- Of those 59 patients, 57 (97%) were subsequently confirmed to have recurrent disease. The NavDx result was the first indication of recurrence, preceding symptoms, clinical exams, and imaging
- Nearly half (48%) of the 80 patients with a positive test had been tested and recurrence identified more than 12 months after completion of definitive therapy
- 97% of asymptomatic patients with a positive NavDx result were subsequently confirmed to have recurrent disease—NavDx detected what clinical exams and imaging had not yet found.
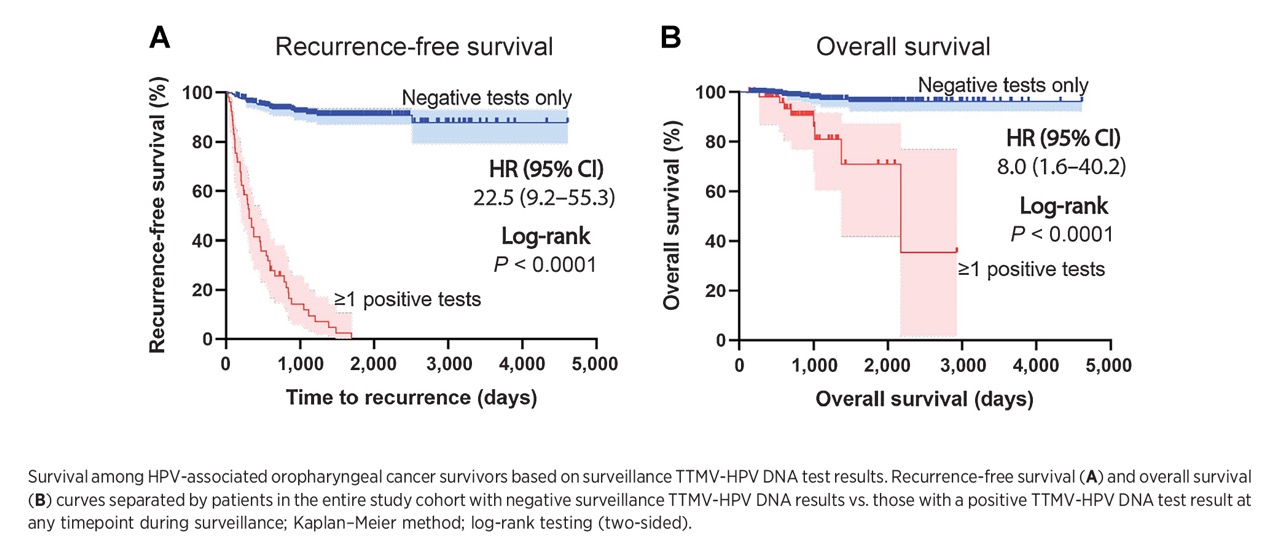
Hanna GJ, Roof SA, Jabalee J, et al. | Clin Cancer Res. 2023 | N=5432
A multi-institutional retrospective observational cohort study of 543 patients evaluated serial TTMV-HPV DNA testing during OPSCC surveillance:
- NavDx testing resulted in few false negatives and few missed recurrences, especially among patients with a known positive result preceding a negative result, with a per-patient NPV of 98.4%
- Recurrence-free and overall survival were significantly worse for patients with any positive TTMV-HPV DNA test result during surveillance. with an estimated recurrence rate 22.5 times higher and chance of survival 8 times lower (p<0.0001)
- NavDx was the first sign of recurrence in 69% of patients with confirmed recurrent disease, with a median lead time of 47–53 days before imaging-confirmed disease
Ferrandino RM, Chen S, et al. | JAMA Otolaryngol Head Neck Surg. 2023 | N=290 (591 tests)1
A single-institution study evaluating NavDx for both diagnosis and surveillance of HPV-associated oropharyngeal cancer. In the surveillance subgroup, NavDx achieved per-test 88.4% sensitivity, 100% specificity, 100% PPV, and 99% NPV, demonstrating exceptional accuracy in a clinical-practice population. Overall diagnostic accuracy was 97.5%.
Roof et al., 2024 | Oral Oncology | N=543, 8 U.S. institutions39
NavDx testing resolved clinically indeterminate surveillance findings (CIFs) with 97.5% accuracy. Positive NavDx results in the CIF setting demonstrated 100% concordance with confirmed recurrence; negative NavDx results showed 96.7% NED confirmation. Median time to diagnosis with a positive NavDx test in the CIF context was 14 days vs. 97.5 days without NavDx testing (p<0.05). CIFs occurred during surveillance of 38.7% of patients, concentrated in year 1 of follow-up.

HPV+ Anal Cancer
NavDx® Testing in Surveillance.
Performance at a Glance.

Standard ASCC Surveillance Has Limitations.
Post-treatment surveillance for HPV+ anal squamous cell carcinoma (ASCC) presents distinct clinical challenges that make molecular monitoring particularly valuable:
-
- Standard ASCC surveillance relies on digital anorectal exam (DARE), anoscopy or high-resolution anoscopy (HRA), and MRI imaging, each with significant limitations in sensitivity, specificity, or accessibility
- Post-chemoradiotherapy (CRT) imaging is typically delayed until approximately 26 weeks post-treatment due to treatment-related inflammation, fibrosis, and tissue changes that make earlier imaging unreliable, creating a window where disease status is uncertain
- Clinically indeterminate findings (CIFs) are common. In the foundational study for NavDx testing in ASCC and its follow-on study, 42-44% of patients experienced at least one CIF during surveillance visits,4,5 resulting in repeat procedures and generating patient anxiety.
- High-resolution anoscopy (HRA), the most sensitive standard tool, is geographically concentrated at specialized centers, creating significant access disparities for patients in rural areas
NavDx testing can provide molecular surveillance during the post-CRT imaging delay and throughout the surveillance period, offering objective disease status information based on a simple blood draw.
Bringing Greater Precision
to HPV+ Cancer Surveillance.
The NavDx Test vs. Standard Surveillance.
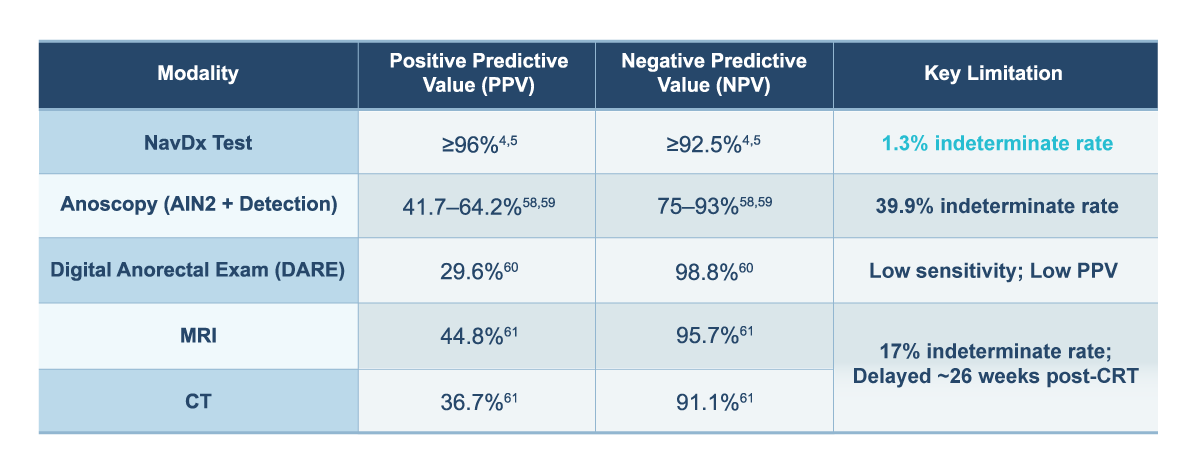
Across two multi-site studies,4,5 standard ASCC surveillance tools generated clinically indeterminate findings (CIFs) in 39–42% of patients. NavDx testing offers a substantially lower indeterminate rate and higher positive predictive value.
Earlier Detection of Recurrence.
Published data demonstrate that NavDx testing can detect molecular evidence of recurrence a median of approximately 2 months earlier than imaging or clinical exam.5 This lead-time advantage has direct clinical implications:
-
- 20-30% of HPV+ ASCC patients experience locoregional or distant recurrence after treatment
- Earlier identification of recurrence may allow intervention while disease burden is still limited. Patients with fewer metastatic lesions at treatment initiation have better long-term outcomes than those with more extensive disease.51
- Earlier identification of recurrence may expand salvage therapy options, including sphincter-preserving limited surgery for the earliest local recurrences, allowing patients to avoid permanent colostomy or additional courses of chemoradiation or brachytherapy.51
Resolving Clinically Indeterminate Findings in ASCC.
Clinically indeterminate findings (CIFs) are one of the most challenging aspects of ASCC surveillance, but NavDx testing can help resolve them. Data from two multi-site studies4,5 show 42-44% of patients had ≥1 CIF during surveillance visits.4,5 Imaging was indeterminate in 17% of visits and clinical exam in 7% of visits. CIF odds were 1.86× higher in year 1 vs. year 2 post-treatment.5 The highest-risk window for recurrence is also when CIFs are most frequent.
- NavDx had an indeterminate rate of 1.3%, or 5-13 times less than standard clinical surveillance methods.5
- NavDx testing resolved CIFs with 92%-94% accuracy with a single test.4,5
- 100% positive concordance was found. Every positive NavDx result performed on a patient with a CIF was found to indicate the presence of a true recurrence.5
- When NavDx testing is positive in a CIF setting, median lead time to confirmed recurrence is 29 days.5
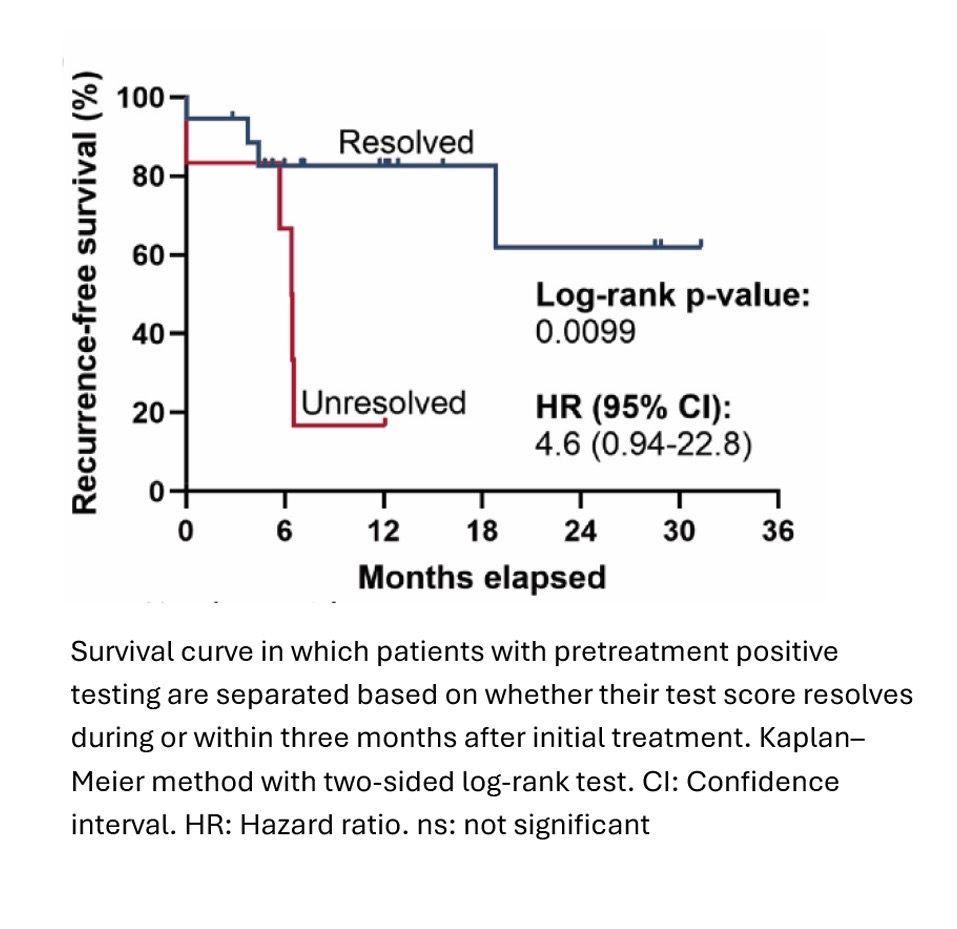
Survival Impact: What a Positive Result Means.
Patients with positive post-treatment NavDx results had significantly worse recurrence-free survival than those with consistently negative test results.4 Consistent negative TTMV Scores during ASCC surveillance is associated with favorable outcomes and provides meaningful clinical reassurance.
Among patients who had a positive pre-treatment NavDx test and were tested again within 3 months post-treatment, 76.0% (19/25) showed resolution of detectable TTMV-HPV DNA. Resolution of positive NavDx results correlated with significantly better recurrence-free survival (p=0.0099, trending toward significance).4
Access and Equity Considerations.
High-resolution anoscopy (HRA), the most sensitive tool for ASCC surveillance, is geographically concentrated at specialized centers, creating significant access disparities for patients in rural areas or those receiving care at HIV care facilities. NavDx testing, requiring only a standard blood draw, may help address this gap by enabling surveillance-quality molecular monitoring at any location where blood can be drawn. Naveris can help arrange patient blood draws outside of your facility to enable access to the NavDx test, wherever your patients are located.
Key Supporting Studies.
Kabarriti R, Lloyd S, Jabalee J, et al. | Cancers (Basel). 2025 | N=117 (368 tests)4
The foundational multi-site NavDx ASCC clinical validation study. 117 patients at 7 U.S. centers; 368 total tests; median follow-up 2 years. 90.6% treated with CRT. HPV16 was the predominant genotype (91.4%). Key findings:
-
- Pre-treatment NavDx detection rate: 85%, establishing TTMV-HPV DNA as a reliable baseline biomarker in ASCC
- Post-treatment per-patient performance: sensitivity 82.8%, specificity 98.4%, PPV 96.0%, NPV 92.5%
- Lead time advantage: median 59 days before imaging or clinical detection of recurrence
- CIF resolution: NavDx correctly classified recurrence status in 33/35 CIF events (94.3%)
- CIF frequency: 44% (52/117) of patients had ≥1 CIF during post-treatment surveillance.
- NavDx indeterminate rate (1.9% (5/267) of tests)
Kabarriti R, Lloyd S, Jabalee J, et al. | Cancers (Basel). 2026 | N=233 (603 tests)5
The dedicated CIF resolution study, the largest multi-site NavDx ASCC study to date. 233 patients at 10 U.S. centers; 603 post-treatment NavDx tests; data January 2020–February 2025. Key findings:
-
- CIF frequency: 42% (90/215) of patients had ≥1 CIF during post-treatment surveillance; 214 total CIFs (46% from exam findings, 54% from imaging)
- Indeterminate rates by modality: Imaging 17%; Clinical exam 7%; NavDx 1.3%
- Overall CIF resolution accuracy: 92% (48/52 evaluable CIF–NavDx pairs)
- CIF resolution: 96% accuracy within 4 months, and 88% after 4 months post-treatment
- When NavDx testing is positive in a CIF setting: 100% concordance with confirmed recurrence; first sign of recurrence in 73% of these patients; median lead time 29 days
- When NavDx testing is negative in a CIF setting: 90% concordance with no recurrence (4/41 false negatives, all locoregional)
- Pre-treatment detection rate: 86.2% (95% CI 78.8–91.7%; N=123 patients)
Huffman BM, et al. | J Immunother Cancer. 2024 | N=2645
A phase II clinical trial analysis evaluating NavDx as a biomarker of pembrolizumab efficacy in advanced ASCC. NavDx TTMV-HPV DNA was detected in 25 of 26 patients with HPV+ ASCC who had pre-treatment testing. Patients who had clinical benefit from pembrolizumab had decreasing TTMV- HPV DNA scores from baseline to 3 and 6 weeks of therapy.
References
- Ferrandino RN, Chen S, Kappauf C, et al. Performance of liquid biopsy for diagnosis and surveillance of human papillomavirus–associated oropharyngeal cancer. JAMA Otolaryngol Head Neck Surg. 2023. http://doi.org/10.1001/jamaoto.2023.1937.
- Hanna GJ, Roof SA, Jabalee J, et al. Negative predictive value of circulating tumor tissue modified viral (TTMV)-HPV DNA for HPV-driven oropharyngeal cancer surveillance. Clin Cancer Res. 2023. http://doi.org/10.1158/1078-0432.CCR-23-1478.
- Berger BM, Hanna GJ, et al. Detection of occult recurrence using circulating tumor tissue modified viral HPV DNA among patients treated for HPV-driven oropharyngeal carcinoma. Clin Cancer Res. 2022. http://doi.org/10.1158/1078-0432.CCR-22-0562.
- Kabarriti R, Lloyd S, Jabalee J, et al. Evaluating tumor tissue modified viral (TTMV)-HPV DNA for the early detection of anal squamous cell carcinoma recurrence. Cancers. 2025. http://doi.org/10.3390/cancers17020174.
- Kabarriti R, Lloyd S, Jabalee J, et al. Resolving clinically indeterminate findings during anal cancer surveillance with TTMV-HPV DNA. Cancers. 2026. http://doi.org/10.3390/cancers18010035.
- Chera BS, Kumar S, Shen C, et al. Plasma circulating tumor HPV DNA for the surveillance of cancer recurrence in HPV-associated oropharyngeal cancer. J Clin Oncol. 2020. http://doi.org/10.1200/JCO.19.02444.
- Chera BS, Kumar S, Beaty BT, et al. Rapid clearance profile of plasma circulating tumor HPV type 16 DNA during chemoradiotherapy correlates with disease control in HPV-associated oropharyngeal cancer. Clin Cancer Res. 2019. https://doi.org/10.1158/1078-0432.CCR-19-0211.
- Rettig EM, Schoenfeld JD, Miller J, et al. A prospective trial of biomarker-guided surveillance for HPV-positive oropharynx cancer using plasma tumor tissue–modified viral HPV DNA. Clinical Cancer Research. 2025. http://doi.org/10.1158/1078-0432.CCR-24-3053.
- Mijares K, Ferrandino R, Chai R, et al. Circulating tumor HPV DNA in patients with head and neck carcinoma: Correlation with HPV genotyping. Am J Surg Pathol. 2024. http://doi.org/10.1097/PAS.0000000000002134.
- Naveris data on file.
- Ho AS, Moyers JT, et al. Evolving use of circulating tumor DNA for HPV+ oropharyngeal carcinoma: Consensus recommendations from the California Head and Neck Consortium. JCO Oncol Pract. 2025. http://doi.org/10.1200/OP-25-00450.
- Surveillance Research Program, National Cancer Institute. SEER*Explorer: An interactive website for SEER cancer statistics [Internet]. 2024.
- Kim JK, Tam M, et al. A phase 2 exploratory trial evaluating computed tomography-based midtreatment nodal response to select for de-escalated chemoradiation therapy in the definitive management of p16+ oropharyngeal cancer. Int J Radiat Oncol Biol Phys. 2026. http://doi.org/10.1016/j.ijrobp.2025.09.054.
- Ferrandino RM, Barlow J, Gold B, et al. Diagnostic accuracy of circulating tumor HPV DNA testing in patients with a lateral neck mass. JAMA Otolaryngol Head Neck Surg.2024. http://doi.org/10.1001/jamaoto.2024.2702.
- Papazian MR, Hicks MD, Mannion K, Turner M, and Topf MC. Diagnostic accuracy of HPV circulating tumor DNA following non-diagnostic FNA of a cystic lateral neck mass. Head Neck. 2026. http://doi.org/10.1002/hed.70060.
- Lambert T, Tasoulas J, Flores M, Sheth S, and Patel S. Circulating tumor HPV DNA as an alternative method to determine HPV status in oropharyngeal squamous cell carcinoma. Oral Oncol. 2023. http://doi.org/10.1016/j.oraloncology.2023.106361.
- Elaldi R, Roussel L-M, Gal J, et al. Correlations between long-term quality of life and patient needs and concerns following head and neck cancer treatment and the impact of psychological distress. A multicentric cross-sectional study. Eur Arch Otorhinolaryngol. 2021. http://doi.org/10.1007/s00405-020-06326-8.
- HPV infection. Mayo Clinic. Updated September 2025. https://www.mayoclinic.org/diseases-conditions/hpv-infection/symptoms-causes/syc-20351596.
- Chen Z, Schiffman M, Herrero R, et al. Classification and evolution of human papillomavirus genome variants: Alpha-5 (HPV26, 51, 69, 82), Alpha-6 (HPV30, 53, 56, 66), Alpha-11 (HPV34, 73), Alpha-13 (HPV54) and Alpha-3 (HPV61). Virology. 2018. http://doi.org/10.1016/j.virol.2018.01.002.
- Division of STD Prevention, CDC. Genital HPV infection fact sheet. https://www.cdc.gov/sti/about/about-genital-hpv-infection.html.
- Human papillomaviruses. IARC Monographs. 2012;100B:255-313.
- American Cancer Society. HPV and cancer. Updated March 2026. https://www.cancer.org/cancer/cancer-causes/infectious-agents/hpv/hpv-and-cancer-info.html.
- Martin, L. Oral HPV and cancer. WebMD. Updated February 2026. https://www.webmd.com/oral-health/guide/oral-hpv-cancer.
- American Cancer Society. Pap Test (Pap Smear). Updated December 2025. https://www.cancer.org/cancer/cervical-cancer/detection-diagnosis-staging/screening-tests/pap-test.html
- Chaturvedi AK, et al. Worldwide trends in incidence rates for oral cavity and oropharyngeal cancers. J Clin Oncol. 2013. http://doi.org/10.1200/JCO.2013.50.3870.
- Kostareli E, Holzinger D, and Hess J. New concepts for translational head and neck oncology: Lessons from HPV-related oropharyngeal squamous cell carcinomas. Front Oncol. 2012. http://doi.org/10.3389/fonc.2012.00036.
- Cancer Research UK. Changes in your appearance due to mouth and oropharyngeal cancer. Updated September 2024. https://www.cancerresearchuk.org/about-cancer/mouth-cancer/living-with/changes-your-appearance
- Fakhry C, Westra WH, Li S, et al. Improved survival of patients with human papillomavirus–positive head and neck squamous cell carcinoma in a prospective clinical trial. JNCI: Journal of the National Cancer Institute. 2008. https://doi.org/10.1093/jnci/djn011.
- Ang KK, Harris J, Wheeler R, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010. https://doi.org/10.1056/NEJMoa0912217.
- Gillison ML, Trotti AM, Harris J, et al. Radiotherapy plus cetuximab or cisplatin in human papillomavirus-positive oropharyngeal cancer (NRG Oncology RTOG 1016): a randomised, multicentre, non-inferiority trial. Lancet. 2019. https://doi.org/10.1016/S0140-6736(18)32779-X.
- Fakhry C et al. Human papillomavirus and overall survival after progression of oropharyngeal squamous cell carcinoma. J Clin Oncol. 2014. https://doi.org/10.1200/JCO.2014.55.1937
- Alemany L, Saunier M, Alvarado-Cabrero I, et al. Human papillomavirus DNA prevalence and type distribution in anal carcinomas worldwide. Int J Cancer. 2015. http://doi.org/10.1002/ijc.28963.
- Eng C, et al. The management and prevention of anal squamous cell carcinoma. Am Soc Clin Oncol Educ Book. 2019. http://doi.org/10.1200/EDBK_237433.
- Barnell GM, Schechter MS. Anal cancer screening and prevention—A new era, limited by access to high-resolution anoscopy. JAMA Netw Open. 2024. http://doi.org/10.1001/jamanetworkopen.2024.0019.
- Rim SH, Saraiya M, Beer L, Tie Y, Yuan X, Weiser J. Access to high-resolution anoscopy among persons with HIV and abnormal anal cytology results. JAMA Netw Open. 2024. http://doi.org/10.1001/jamanetworkopen.2024.0068.
- Rim SH, Beer L, Saraiya M, Tie Y, Yuan X, and Weiser J. Prevalence of anal cytology screening among persons with HIV and lack of access to high-resolution anoscopy at HIV care facilities. J Natl Cancer Inst. 2024. http://doi.org/10.1093/jnci/djae094.
- Ghodraty Jabloo V, Alibhai SMH, Fitch M, Tourangeau AE, Ayala AP, and Puts M. Antecedents and outcomes of uncertainty in older adults with cancer: A scoping review of the literature. Oncol Nurs Forum. 2017. http://doi.org/10.1188/17.ONF.E152-E167.
- Bergerot CD, et al. Fear of cancer recurrence or progression: What is it and what can we do about it? Am Soc Clin Oncol Educ Book. 2022. http://doi.org/10.1200/EDBK_100031.
- Roof SA, Jabalee J, Rettig EM, Chennareddy S, Ferrandino RM, Chen S, Posner MR, Genden EM, Chai RL, Sims J, Thrash E, Stern SJ, Kalman NS, Yarlagadda S, Raben A, Clements L, Mendelsohn A, Kaczmar JM, Pandey Y, Bhayani M, Del Vecchio Fitz C, Hanna GJ. Utility of TTMV-HPV DNA in resolving indeterminate findings during oropharyngeal cancer surveillance. Oral Oncol. 2024. http://doi.org/10.1016/j.oraloncology.2024.106874.
- Hollander A, Nonaka T. Cell-free HPV-DNA as a high-accuracy biomarker for treatment de-escalation in HPV-positive head and neck squamous cell carcinoma. Front Oncol. 2025. http://doi.org/10.3389/fonc.2025.1569877.
- Bastien AJ, Ng J, Cong I, Garcia J, Walgama ES, Luu M, Jang JK, Mita AC, Scher KS, Moyers JT, Mallen-St. Clair J, Maghami E, Chen MM, Zumsteg ZS, and Ho AS. Patient perceptions underlying ctDNA molecular surveillance for HPV(+) oropharyngeal squamous cell carcinoma. Oral Oncol. 2024. https://doi.org/10.1016/j.oraloncology.2024.106894.
- Lin MG, Zhu A, Read PW, Garneau J, and McLaughlin C. Novel HPV associated oropharyngeal squamous cell carcinoma surveillance DNA assay cost analysis. Laryngoscope. 2023. http://doi.org/10.1002/lary.30701.
- Gupta T, Master Z, Kannan S. et al. Diagnostic performance of post-treatment FDG PET or FDG PET/CT imaging in head and neck cancer: A systematic review and meta-analysis. Eur J Nucl Med Mol Imaging. 2011. http://doi.org/10.1007/s00259-011-1893-y.
- Lang Kuhs KA, Brenner JC, Holsinger FC, and Rettig EM. Circulating tumor HPV DNA for surveillance of HPV-positive oropharyngeal squamous cell carcinoma: A narrative review. JAMA Oncol. 2023. http://doi.org/10.1001/jamaoncol.2023.4042.
- Huffman BM, Singh H, Ali LR, Horick N, Wang SJ, Hoffman MT, et al. Biomarkers of pembrolizumab efficacy in advanced anal squamous cell carcinoma: analysis of a phase II clinical trial and a cohort of long-term responders. Journal for ImmunoTherapy of Cancer. 2024. http://doi.org/10.1136/jitc-2023-008436.
- Kais A, Santiago SP, Han PC, Clump DA, Stokes WA, Fancy T, Cui R, Martin E and Turner MT. Human papillomavirus circulating tumor DNA: a diagnostic tool in squamous cell carcinoma of unknown primary-a pilot study. Front Oncol. 2024. http://doi.org/10.3389/fonc.2024.1376595.
- Rettig EM, Wang AA, Tran N, et al. Association of pretreatment circulating tumor tissue-modified viral HPV DNA with clinicopathologic factors in HPV-positive oropharyngeal cancer. JAMA Otolaryngol Head Neck Surg. 2022. Article: http://doi.org/10.1001/jamaoto.2022.3282. Erratum: http://doi.org/10.1001/jamaoto.2022.4289.
- Ellsworth G, Shen R, Marcelin K-A, Majumdar R, Bazil M, Moore G, Nelson M, Alland I, Sepulveda G, Wilkin T, and Higginson D. High specificity of HPV cell-free DNA tests in persons with HIV for the detection of HPV-related cancer. J Acquir Immune Defic Syndr. 2023. http://doi.org/10.1097/QAI.0000000000003231.
- Routman DM, Kumar S, Chera BS, Jethwa KR, Van Abel KM, Frechette K, DeWees T, Golafshar M, Garcia JJ, Price DL, Kasperbauer JL, Patel SH, Neben-Wittich MA, Laack NL, Chintakuntlawar AV, Price KA, Liu MC, Foote RL, Moore EJ, Gupta GP, and Ma DJ. Detectable postoperative circulating tumor human papillomavirus DNA and association with recurrence in patients with HPV-associated oropharyngeal squamous cell carcinoma. Int J Radiat Oncol Biol Phys. 2022. http://doi.org/10.1016/j.ijrobp.2022.02.012.
- Huttinger ZM, Gogineni E, Baliga S, Blakaj DM, Bhateja P, Bonomi M, Kang SY, Old MO, Seim NB, VanKoevering KK, Agrawal A, Ozer E, Rocco JW, and Haring CT. Circulating tumor DNA determines induction chemotherapy response in HPV associated oropharyngeal squamous cell carcinoma: A pilot study. Oral Oncol. 2025. http://doi.org/10.1016/j.oraloncology.2025.107179.
- Frazer ML, Yang G, Felder S, McDonald J, Sanchez J, Dessureault S, Imanirad I, Carballido E, Kim R, Hoffe S, and Frakes J. Determining optimal follow-up for patients with anal cancer following chemoradiation. Am J Clin Oncol. 2020. http://doi.org/10.1097/COC.0000000000000673.
- Chung CH, Li J, Steuer CE, Bhateja P, Johnson M, Masannat J, Poole MI, Song F, Hernandez-Prera JC, Molina H, Wenig BM, Kumar S, Kuperwasser C, Stephens PJ, Farinhas JM, Shin DM, Kish JA, Muzaffar J, Kirtane K, Rocco JW, Schell MJ, Saba NF, and Bonomi M. Phase II multi-institutional clinical trial result of concurrent cetuximab and nivolumab in recurrent and/or metastatic head and neck squamous cell carcinoma. Clin Cancer Res. 2022. http://doi.org/10.1158/1078-0432.CCR-21-3849.
- Cabel L, Jeannot E, Bieche I, Vacher S, Callens C, Bazire L, Morel A, Bernard-Tessier A, Chemlali W, Schnitzler A, Lièvre A, Otz J, Minsat M, Vincent-Salomon A, Pierga J-Y, Buecher B, Mariani P, Proudhon C, Bidard F-C, and Cacheux W. Prognostic impact of residual HPV ctDNA detection after chemoradiotherapy for anal squamous cell carcinoma. Clin Cancer Res. 2018. http://doi.org/10.1158/1078-0432.CCR-18-0922.
- Bernard-Tessier A, Jeannot E, Guenat D, Debernardi A, Michel M, Proudhon C, Vincent-Salomon A, Bièche I, Pierga J-Y, Buecher B, Meurisse A, François E, Cohen R, Jary M, Vendrely V, Samalin E, El Hajbi F, Baba-Hamed N, Borg C, Bidard F-C, and Kim S. Clinical validity of HPV circulating tumor DNA in advanced anal carcinoma: An ancillary study to the epitopes-HPV02 trial. Clin Cancer Res. 2019. http://doi.org/10.1158/1078-0432.CCR-18-2984.
- Wong ET, Dmytriw AA, Yu E, et al. 18F-FDG PET/CT for locoregional surveillance following definitive treatment of head and neck cancer: A meta-analysis of reported studies. Head & Neck. 2019. https://doi.org/10.1002/hed.25513
- Masroor F, Corpman D, Carpenter DM, Ritterman Weintraub M, Cheung KHN, and Wang KH. Association of NCCN-recommended posttreatment surveillance with outcomes in patients with HPV-associated oropharyngeal squamous cell carcinoma. JAMA Otolaryngol. Neck Surg. 2019. https://doi.org/10.1001/jamaoto.2019.1934.
- Su W, Rajeev-Kumar G, Kang M, et al. Long-term outcomes in patients with recurrent human papillomavirus-positive oropharyngeal cancer after upfront transoral robotic surgery. Head & Neck. 2020. https://doi.org/10.1002/hed.26396
- Gimenez F, Costa-e-Silva IT, Daumas A, Araújo, Jd, Medeiros SG, and Ferreira, L. The value of high-resolution anoscopy in the diagnosis of anal cancer precursor lesions in HIV-positive patients. Arq. Gastroenterol. 2011. https://doi.org/10.1590/S0004-28032011000200010
- Brenes D, Kortum A, Carns J, Mutetwa T, Schwarz R, Liu Y, Sigel K, Richards-Kortum R, Anandasabapathy S, Gaisa M, and Chiao, E. Automated in vivo high-resolution imaging to detect human papillomavirus–associated anal precancer in persons living with HIV. Clinical and Translational Gastroenterology. 2023. http://doi.org/10.14309/ctg.0000000000000558
- Ang CW, Dawson R, Hall C, and Farmer M. The diagnostic value of digital rectal examination in primary care for palpable rectal tumour. Colorectal Disease. 2008. https://doi.org/10.1111/j.1463-1318.2007.01381.x
- Adusumilli P, Elsayed N, Theophanous S, Samuel R, Cooper R, Casanova N, Tolan DJ, Gilbert A, and Scarsbrook AF. Combined PET-CT and MRI for response evaluation in patients with squamous cell anal carcinoma treated with curative-intent chemoradiotherapy. Eur Radiol. 2022. http://doi.org/10.1007/s00330-022-08648-z.
- Eng C, Ciombor KK, Cho M, Dorth JA, Rajdev LN, Horowitz DP, Gollub MJ, Jácome AA, Lockney NA, Muldoon RL, Washington MK, O’Brian BA, Benny A, Lebeck Lee CM, Benson AB 3rd, Goodman KA, and Morris VK. Anal cancer: Emerging standards in a rare disease. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2022. http://doi.org/10.1200/JCO.21.02566.
- Littlejohn JB, and Brister KA. Management of Recurrent Anal Cancer. Oncol. Clin. 2025. https://pubmed.ncbi.nlm.nih.gov/39547772/
- Upadhyay L, Hartzell M, Parikh AR, Strickland MR, Klempner S, and Malla M. Recent advances in the management of anal cancer. Healthcare. 2023. https://doi.org/10.3390/healthcare11233010